Cruel and Unusual Punishment
Since abortion has been legalized there have been many techniques
promoted to end the life of a developing unborn child. The following are
methods used to perform abortions and possible complications from the
procedures.
First Trimester (
The first trimester ends when the baby is about 12 weeks old.)
Suction Curettage (Vacuum Aspiration)- This is the most extensively used abortion technique, especially
during first trimester abortions. It is performed in approximately 97% of abortion procedures(1) . In this
procedure, the cervix is dilated by a group of instruments. A powerful suction tube with a knife-like edge on
the tip is inserted into the uterus. The suction or vacuum dismembers the unborn child and sucks her out of
the womb. The abortionist must also use his tool to remove the placenta, blood, and amniotic fluid.
Complications of Suction Curettage- The most frequent post-abortion complication is infection. Infection
can occur if any of the fetal or placental tissue is left in the uterus(2) . Another possible complication is uterine
hemorrhage. Hemorrhaging can occur if the uterus is punctured during the abortion(3) .
Dilatation and Curettage (D&C)- In this abortion method, the cervix is dilated so a steel knife with a loop
shape can be inserted into the uterus. The abortionist then uses this knife to scrape the wall of the uterus.
This scraping cuts the unborn child to pieces and removes both the child and placenta from the uterine wall.
Complications from D & C- The most apparent complication from this procedure is extensive bleeding.
Other common complications include infection and uterine perforation(4) .
RU486 (Abortion Pill)- RU486 is a combination of two drugs used to expel a child from the womb. During
the first visit to the abortion clinic, a woman will take mifepristone orally. Mifepristone blocks natural
hormones that maintain the nutrient rich lining of the uterus. The developing baby dies as the lining of the
uterus disintegrates. On the second visit to the doctor, the woman takes misoprostol, which was originally
designed as an ulcer medicine, to produce powerful contractions. After taking this drug, most women abort
within 4 hours, but 30 percent abort their children later at work, home, etc(5) . On the third visit to the clinic, the
abortionist will confirm the death of the unborn child and check for complications.
Complications of RU486- In the clinical trials performed in the U.S. on 2,121 women from September 1994
to September 1995, a large number of complications were documented. The New England Journal of Medicine
reported these findings: the most frequent side effects were bleeding and cramping; nausea and vomiting
were also frequent; 56 women underwent surgical intervention for excessive bleeding; 4 women received
blood transfusions; the average duration of bleeding was 13 days, and 170 women or 8 percent of the women
didnít abort their unborn children and were encouraged to have a surgical abortion(6) . On September 24, 1995,
the Waterloo Courier (Iowa) printed a letter from Dr. Mark Louviere, in which he described a women who
lost half her blood and almost died from RU-486 complications. It should also be noted that there havenít
been any long-term effects studies done with these drugs so no one is certain if there are any possible longterm
side effects from using these two drugs.


Second Trimester (
The Second Trimester (13-28 Weeks)
Salt Poisoning (Saline Amniocentesis)-After 16 weeks-In this procedure, a needle with a solution of
concentrated salt is inserted through the womanís abdomen into the amniotic sac. The child breathes in the
salt and is poisoned. It usually takes around an hour for the unborn child to die. After 33 to 35 hours the
woman goes into labor and delivers a dead, shriveled baby(7) .
Complications of Salt Poisoning- One possible side effect of salt poisoning is that the mother might get a
condition called consumption coagulopathy, which is uncontrolled blood clotting throughout the body, with
severe hemorrhaging and other serious side effects to the nervous system(8) . If the abortionist misses the
womb and injects the saline solution into the womanís vascular system, seizures, coma, or death can result(9) .
This procedure is outlawed in Japan and other countries because of these risks to the woman(10) .
Dilation and Evacuation (D & E) -12 to 24 weeks- This procedure was developed since salt poisoning was
considered too dangerous and has largely replaced it as the second-trimester abortion procedure(11) . In this
method, the cervix is dilated so grasping forceps can be inserted into the uterus. At this stage in development,
the childís bones have hardened, so the baby can no longer be removed by suction or scraping. The abortionist
uses these forceps to dismember different parts of the child, such as arms and legs. The childís head is
often too large to be removed from the womb, so the abortionist must crush the skull in order to remove it.
When the procedure is over, a nurse will attempt to reassemble the body parts to make sure that there is
nothing left in the uterus.
Complications of D & E-Bleeding is usually profuse and infection can occur if the abortionist doesnít
remove all of the pieces of the childís body from the womb. This procedure, along with D & C, is performed
blindly with the abortionist using only his or her sense of feel. If an abortionist isnít careful, the uterus,
bladder, and bowels can be punctured.
Third Trimester
(27 - 40 weeks)
Partial-Birth Abortion (D & X)-20 weeks and beyond-This is a three day procedure. During the first two
days, the pregnant womanís cervix is anesthetized and dilated. On the day of the operation, the abortionist
uses a sonogram to find the childís leg. Once the abortionist has a hold of a leg with forceps, the child is
pulled through the birth canal until the whole child is delivered except for the head. The abortionist then
forces scissors into the base of the skull and spreads the scissors so a suction catheter can be put into this hole
and evacuate the contents of the skull(12) .

Complications of D & X- In order to unnaturally dilate a women's cervix, an abortionist must insert laminaria,
a few at a time, over a 3 to 5 day period. This unnatural dilatation can cause various complications
such as large amounts of pain, infection, and an incompetent cervix, which makes it difficult for women to
have children in the future. Complications that are possible when the abortionist is reaching for the childís
foot include hemorrhage, uterine perforation, uterine rupture, amniotic fluid embolus, and trauma to the
uterus. The complications that are possible when the abortionist blindly inserts scissors into the childís skull
are laceration of the uterus or cervix by the scissors and could result in severe bleeding and the threat of
shock or even maternal death(13).
Specialized Abortion Procedure
Fetal Reduction- With the use of in-vitro fertilization, a specialized form of abortion is being used. This form
of abortion is called fetal reduction. When a woman attempts to become pregnant with in vitro fertilization,
usually multiple embryos are placed in her womb. This method, which increases the probability of pregnancy
also increases the probability of a multiple pregnancy. Women who become pregnant with more than two
children can elect for fetal reduction. During a fetal reduction procedure, a needle is inserted into the heart of
the unborn child. The child is then injected with potassium chloride (a saline solution) and dies. The leasthealthy
looking or easiest to kill fetuses are usually reduced.


Overview of Complications
Early Complications. The following are complications for women which may be identified a few
weeks after an abortion.
Bleeding: In many women, the bleeding is so profuse that blood transfusions are required.
Infection: The damage done can range from mild to fatal. Compared to hospitals, the rate of infections in
abortion clinics with far inferior care is at least doubled(14). The usual infection is called pelvic inflammatory
disease (PID). PID is difficult to control and can lead to sterility even when there is prompt treatment. Some
women with PID can have chronic pain for the rest of their lives(15) .
Failure to remove parts of the child: If an abortionist leaves part of a child inside the womb during an
abortion, severe infection may result. This infection would cause severe cramping and bleeding, and if the
infection persists, the woman may have to have a hysterectomy (removal of the womb).
Embolisms: Since abortion is an unnatural procedure that the body isnít ready for, the slicing of the placenta
from the uterine wall can cause fluids around the child, pieces of tissue, or blood clots to enter the womanís
circulation. These then travel to the lungs of the woman causing damage and occasionally death(16) .
Long-Term Complications. Many of the complications from abortion might not be seen until years
after the abortion takes place and might not even be recognized as complications of abortion.
Ectopic Pregnancy: An ectopic pregnancy occurs when an embryo implants at a site other than the lining of
the uterus. The child will continue to grow in a place outside of the womb, often in the fallopian tube.
Surgery is then required to remove the child, in order to save the mother.
Studies have shown that women who abort their first pregnancy increase their risk of having an ectopic
pregnancy by 500%(17) . Centers for Disease Control reports that about 100,000 ectopic pregnancies occur each
year which is a rise of over 500% since the pre-Roe v. Wade number of 17,800 in 1970. The CDC also reports that
ectopic pregnancies are the leading cause of pregnancy-related deaths in the first trimester and account for 9% of
all pregnancy-related deaths in this country. (î)
Increase in Miscarriages and Other Pregnancy Complications: Studies have shown that abortion during
the first pregnancy can cause significant increases in complications with later pregnancies(18).
Another study shows that pregnancy failure is increased 45% if a woman has had one previous abortion(18) .
Other studies showed that premature births, neonatal deaths, and miscarriages in the first and second trimesters
of pregnancy were significantly increased in women who had experienced an induced abortion(20, 21, 22).
Breast Cancer: In studies across the United States and in other countries, it has been found that women who
have had abortions have a higher chance of getting breast cancer later in life. These are studies that have
been done by professionals and are published in respected medical journals.
One study, done in 1990, that summarized findings in medical studies from Canada, Denmark,
France, Israel, Japan, the United States, and the USSR, found that ìabortions, either multiple or occurring
before the first full term pregnancy, have been shown to be significantly associated with breast
cancer risks(23.î) A study done by the National Cancer Institute in Washington found that women who had
an abortion increased their risk of getting breast cancer by 50%. This risk was more than doubled if the
womanís abortion (or first abortion) took place before the age of 18 or over the age of 30(24).
Abortion's link to breast cancer is theorized to exist because abortion is an unnatural procedure
which stops the natural condition of a womanís breasts getting ready to produce milk for her child. In
early pregnancy, a womanís breast tissue grows and begins to differentiate to cells that will produce
milk. An abortion stops this natural process, so many of the cells that would have produced milk are
now undifferentiated cells. These cells are much more capable of turning into cancer cells then the cells
that were present before she became pregnant.
Sterility: Other complications of abortion, such as infections, can often cause scar tissue in the
womb. If the scar tissue covers the opening between the uterus and the fallopian tubes, it is impossible
for a sperm to fertilize a woman's egg. If fertilization can't occur then a woman can't become
pregnant through natural means.
Psychological Consequences: Although a woman might not be harmed physically by an abortion, there is a
good possibility that she could be hurt psychologically. Research is providing evidence that having an
abortion can have negative psychological effects. Researchers have found that at least 19% of post-aborted
women suffer from symptoms such as, but not limited to: feelings of intense grief or depression because of
the abortion, anxiety attacks, difficulty concentrating, irritability, flashbacks to the abortion experience,
recurrent thoughts about their aborted child, and nightmares or sleeping disorders(25). The term for this specific
group of symptoms is post-abortion syndrome or PAS. PAS has been proposed as a subset of PTSD (posttraumatic
stress disorder). People who have PTSD often try to suppress their feelings about a traumatic
event. They often want to, but are unable to, express their feelings and emotions about this event.
Women
with PAS will often do whatever they can to get rid of their feelings of guilt, including drug and alcohol use.
Even though some abortions are performed without complications, there is no such thing as a safe
abortion. In every successful abortion, an innocent child dies. The woman might not always be harmed but
the child always is.
References:
1CDCís Abortion Surveillance 1997.
2Jane E. Hodgson, M.D., ìAbortion by Vacuum Aspiration,î Abortion and Sterilization: Medical and Social
Aspects, Jane E. Hodgson, ed., (New York: Academic Press, Grune and Strathon, 1981), pp. 256, 260-261.
3Ibid, pp. 256-258.
4Gary F. Cunningham, M.D., et. al, Williams Obstetrics, 19th ed., (Norwalk, CT: Appleton & Lang, 1993), p.
683.
5Population Council of New York, Release, October 27, 1994, p. 3.
6Irving M. Spitz, C. Wayne Bardin, Lauri Benton, Ann Robins, ìEarly Pregnancy Termination with
Mifepristone and Misoprostol in the United States,î New England Journal of Medicine, Vol. 338, No. 18
(April 30, 1998), pp. 1241-1247.
7Stephen L. Corson., M.D., et al, Fertility Control, (Boston: Little, Brown, and Company, 1985), pp. 82-83.
8James R. Scott, M.D., et al, Danforthís Obstetrics and Gynecology, 6th ed.,(Philadelphia: J.B. Lippincott, 1990),
p. 726.
9R. Bolognese and S. Corson, Interruption of Pregnancyñ A Total Patient Approach, (Baltimore: Wilkins and
Wilkins, 1985), p. 136.
10Thomas D. Kerenyi, Abortion and Sterilization: Medical and Social Aspects, edited by Jane E. Hodgson,
(New York: Academic Press Grune and Strathon, 1981), p. 360.
11Dr. and Mrs. J.C. Willke, Why canít We Love them Both, (Cincinnati: Hayes Publishing Company, 1997), p.
120.
12Martin Haskell, M.D., ìDilation and Extraction for Late Second Trimester,î in ìSecond Trimester Abortion:
From Every Angle,î Fall Risk Management Seminar, September 13-14, 1992, Dallas, Texas, National Abortion
Federation.
13M. LeRoy Sprang, MD and Mark G. Neerhof, ìRationale for Banning Abortions Late in Preg-
nancy,î Journal of the American Medical Association, volume: 280, August 26, 1998, p. 744.
14C. Gassner and C. Ballard, American Journal Obstetrics and Gynecology, vol. 48, p. 716.
15M. Spence, ìPID: Detection and Treatment,î Sexually Transmitted Disease Bulletin, Johns Hopkins University,
vol. 3, no 1, February 1983.
16W. Cates, et al., American Journal Obstetrics and Gynecology, vol. 132, p. 16.
17Chung, et al., ìEffects of Induced Abortion Complications on Subsequent Reproductive Function,î U. of
Hawaii, Honolulu.
18Stanislaw Leinbrych, M.D., ìFertility Problems Following Aborted First Pregnancy,î New Perspectives On
Human Abortion, edited by Hilgers, Horan, Mall, (Frederick, Maryland; University Publication of America,
1981) pp. 120-134.
19C. Madore, et. al., ìA Study on the Effects of Induced Abortion on Subsequent Pregnancy Outcome,î
American Obstetrics and Gynecology, 1981, vol. 139, pp. 516-521.
20American Journal of Epidemiology, Vol. 102, No. 3, 1975, pp. 217-224.
21Wright, et. al., Lancet, June 10 1972, 1, pp. 1278-1279.
22J. Richardson and G. Dixon, British Medical Journal, 1976, 1, pp. 1303,-1304
23L. Remennick, ìInduced Abortion as a Cancer Risk Factor: A Review of Epidemiological Evidence,î
Journal of Epidemiological Community Health, 1990, 44: 259-264.
24J.R. Daling., K.E. Malone, L.F. Voight, E. White, and N.S. Weiss, ìRisk of Breast Cancer Among Young
Women: A Relationship to Individual Abortion,î Journal of the National Cancer Institute, 1994, 86: 1584-
1592.
25C. Barnard, The Long-Term Psychological Effects of Abortion, (Portsmouth,N.H: Institute for Pregnancy
Loss, 1990).
Abortion and the Bible
Chronology of a New Life
The life of a baby begins, of course, long before birth. Every new and unique human being begins his or her life at the moment of fertilization and, if not interrupted, will someday grow into an adult man or woman. Following are some facts of our earliest days of life, recognized in medical texts as well as basic biology books.
First Month
The sperm joins the ovum (egg) to form one cell. This one cell contains the complex genetic blueprint for every detail of human development - sex, hair and eye color, height, skin tone, etc. Over the next week the tiny fertilized egg (or blastocyst) travels down the fallopian tube into the uterus, implanting in the nutrient-rich lining which has been prepared by the hormone progesterone. The embryo begins developing very rapidly, and by 22 days the heart begins to beat. By the end of the third week the backbone, spinal column and nervous system are developing. Kidneys, the liver and the digestive tract are already taking shape. By the end of the first month the embryo is ten thousand times larger than at the blastocyst stage. This tiny baby has grown to about 1/4 of an inch in length.
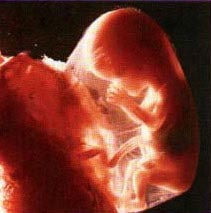
Second Month
At this stage of development the head of the embryo is almost one half of his or her total size. Brain tissues grow rapidly, dividing and becoming a miniature brain that is distinctly human. By 40 days (the sixth week) brain waves can be recorded. Fingers and feet are beginning to develop. Milk teeth form at 61/2 weeks. Facial features, including ears, nose, lips and tongue, form with clarity during this month. Eyes form and darken when pigment is produced around day 35. Eyelids cover the eyes and will soon form a protective seal, reopening during the seventh month. Near the end of the month the skeleton changes from cartilage to bone. Forty muscle sets begin their first exercises and, working with the nervous system, respond with small movements to touch. The baby's blood type is often different from his or her mother's. By eight weeks all body systems are present, and from now on changes will be primarily in size and refinement of body parts already formed. The tiny baby at this stage is called a fetus, Latin for "offspring" or "young one."
Third Month
During this month the baby grows to a length of more than two inches and a weight of one ounce. At nine weeks fingerprints are evident and never change. The baby now sleeps, awakens and exercises muscles energetically - turning the head, curling toes and opening and closing his or her mouth. The palm, when stroked, will make a tight fist. Fingernails and toenails form, and the baby's sex is now identifiable. The baby breathes amniotic fluid to help develop and strengthen the respiratory system. Vocal cords are complete, and at times it appears as if this little baby is crying.
Fourth Month
Rapid growth during this month - the baby grows to eight to ten inches in length and weighs a half pound or more - means the mother often begins to show and may feel her baby move. Bone marrow is forming, and the heart can be plainly heard as it pumps up to 25 quarts of blood each day. Nutrients in food consumed by the mother are passed on to her baby within an hour or two via placenta and umbilical cord - which is transporting three hundred quarts of fluid per day! Facial expressions similar to the baby's parents can be identified at this time. Fine hair begins growing on the head, eyebrows and eyelashes. The baby learns to grip and suck his or her thumb.
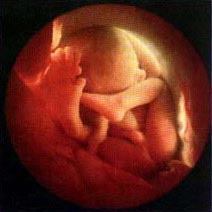
Fifth Month
Half the pregnancy has now passed and this little baby is very active! Sleeping habits develop and the mother often feels her baby move and stretch, particularly when she is resting. Interestingly, babies at this stage have responded to sounds in frequencies too high and low for adults to hear. By the end of this month the baby is about 12 inches long and weighs about one pound. Babies born at this stage of development have survived.
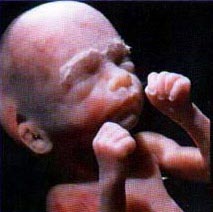
Sixth Month
The baby, now up to 14 inches long and a pound and a half in weight, can now roll over inside the womb. Oil and sweat glands are functioning and the baby is covered by a white filmy layer called vernis (Latin for "varnish") which protects the delicate skin from the surrounding amniotic fluid. At the end of this month the baby has completed two-thirds of his or her stay in the womb and because the lungs are fairly well-developed would stand a good chance of survival if born at this time.
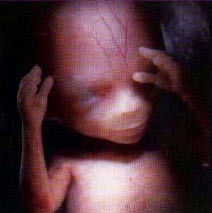
Seventh Month
The baby weighs at least two pounds by the seventh month. All four senses are now used, the eyelids open and close, and eyes look around. The baby can taste, touch and recognize his or her mother's voice. Eye teeth are present within the baby's gums, and this little baby's hands develop an even stronger grip. During the last trimester the baby receives antibodies from the mother through the placenta that will provide immunity to a wide variety of diseases.
Eighth Month
The skin begins to thicken with a layer of fat stored beneath for insulation and nourishment. Antibodies to give immunity against disease are continuing to be received from the mother, strengthening and preparing this baby for life outside the womb. The baby absorbs a gallon of amniotic fluid per day; the fluid is completely replaced every three hours. During this month the baby gains at least two pounds, doubling his or her weight, and the mother is probably looking forward to the delivery date!
Ninth Month
By the ninth month, weighing six to nine pounds, this baby can only turn from side to side because of very cramped quarters. At this point most babies settle into a head-down position to prepare themselves for delivery. About a week before birth, growth stops and changes in the mother's hormonal balance signal the onset of labor and birth. Over the past nine months, one cell has become two hundred million cells, weighing six billion times more than at fertilization, yet containing - in a bit greater detail - the same unique person that came into being at that first moment!
Details provided in this chronology are taken from The First Nine Months of Life by Geraldine L. Flanagan and When You Were Formed in Secret by Gary Bergel.
Goodbye Taylor
Back to KJV Of GOD'S WORD The Good News of God's Word! Abortion and the Bible